Dr. Felix Berger, Universitatsmedizin Berlin, discussed treatment of atrial septal defect (ASD) with interventional closure. The Amplatzer occluder is the easiest device to use, has the best closure with the lowest embolization rates, and can be used for defects up to 40 mm using a standardized procedure. The introduction of the Amplatzer occluder in 1997 led to an increase in yearly rates of interventional ASD closure from about 25% to 70-80%. Nearly 40% of patients treated with interventional closure are >20 years old, with a significant number over age 60. ASD >20 mm diameter accounts for 32.2% of ASD in adults versus 5.6% in children. ASD in adults also is a more complex disease than in pediatric patients (Figure 1).
|
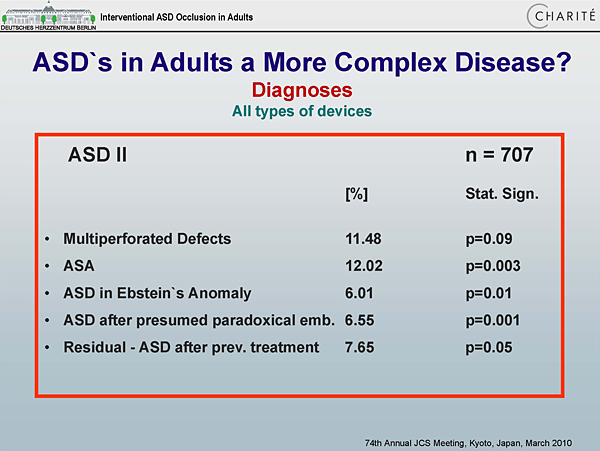
Figure 1. ASDs in Adults a More Complex Disease?
【Click to enlarge】 |
|
|
|
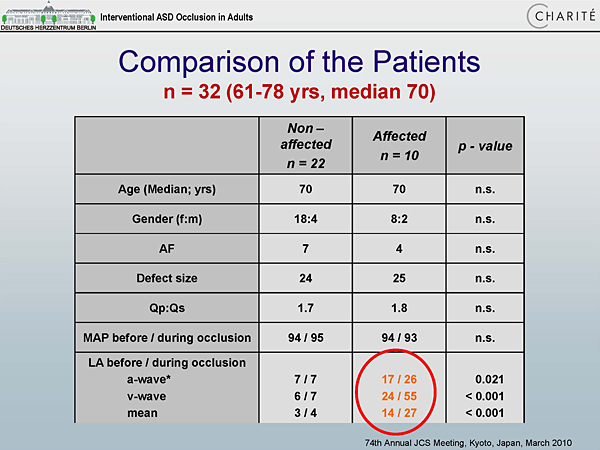
Figure 2. Comparison of Patients.
【Click to enlarge】 |
|
|
|
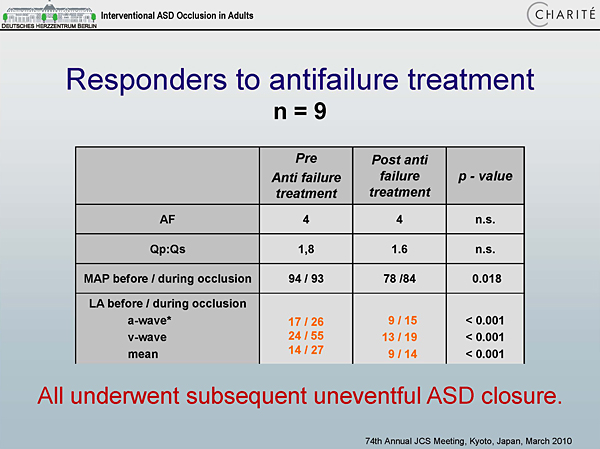
Figure 3. Responders to Antifailure Treatment.
【Click to enlarge】 |
|
|
|
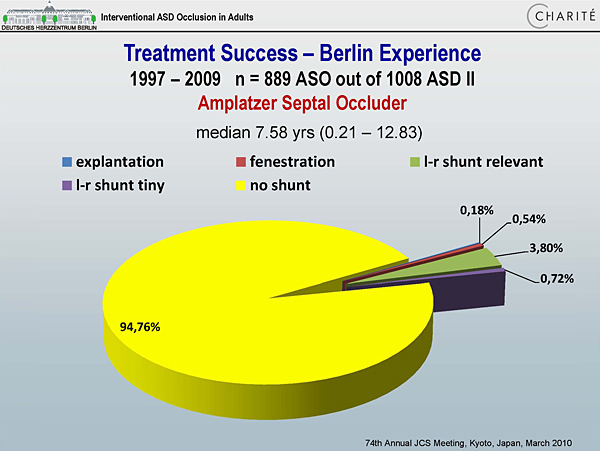
Figure 4. Treatment Success – Berlin Experience
【Click to enlarge】 |
|
|
|
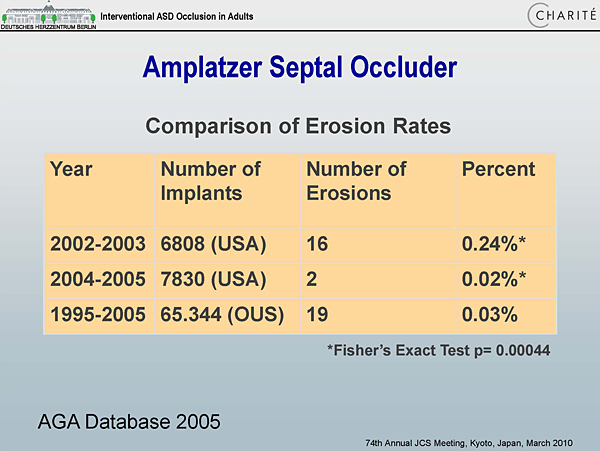
Figure 5. Amplatzer Septal Occluder.
【Click to enlarge】 |
|
|
In selected cases it is possible to close defects >40 mm. For multiperforated or multiple defects, simultaneous balloon sizing is necessary. If the distance between the perforations is >6-7 mm, a second device is required; if <6-7 mm, a single occluder can be used. In elderly patients with elevated left atrial (LA) pressure, the ASD may have a decompressive impact on the left ventricle (LV).
Older patients with diastolic dysfunction have significantly higher LA pressure than those without diastolic dysfunction (Figure 2). Diastolic function can be improved by pretreatment with diuretics and ACE inhibitors, with or without beta-blockers. Nine patients who responded to pretreatment had significantly lower LA pressure after pretreatment and underwent successful ASD closure (Figure 3). A self-made fenestrated device was used in non-responders, to allow decompression of the LV after occlusion.
Several studies have demonstrated better preservation of cardiac function and lower incidence of arrhythmias with device closure versus surgery. Among 889 patients treated with the Amplatzer occluder, a 94.76% total occlusion rate was achieved (Figure 4). The occlusion rate was 98% in patients with a single secundum ASD compared with 81% in patients with multiperforated ASD and 87% in those with complex CHD.
Potential complications of interventional closure are embolization/migration (0.025%) and erosion of the atrial roof or aortic root. According to Dr. Berger, performance of Nitinol devices is the major cause of erosion. Figure 5 compares erosion rates from different databases. In a multicenter retrospective analysis, complication rates of interventional closure versus surgery were 1.6% versus 5.2% for major complications (p=0.03) and 6.1% versus 18.8% for minor complications (p <0.001).
In conclusion, interventional closure of defects up to 40 mm diameter is quick, safe, and effective, with a success rate similar to surgery and a low complication rate.
|