Ulrich Sigwart, MD, University of Geneva, discussed the current treatment of hypertrophic obstructive cardiomyopathy (HOCM). HOCM is characterized by hypertrophy of the left ventricle outflow tract (LVOT). Therapeutic approaches have been centered around eliminating this greatly enlarged area of the heart. HOCM typically creates an enormous LVOT gradient (LVOTG) with low aortic pressures and extremely high LV apical pressures, which in turn elevates the filling pressure up to about 40 mmHg.
Symptoms include chest pain, dyspnea, pulmonary congestion, palpitations, syncope, and sudden death. Treatment typically begins with negative inotropes, followed by pacing or defibrillator. When these approaches fail, outflow tract enlargement should be considered before transplantation. Methods of outflow tract enlargement include transthoracic surgical myectomy and ablation to induce shrinkage.
Myectomy is effective but requires major surgery, extracorporeal circulation, and a steep learning curve. For these reasons, transluminal approaches for septal ablation have been investigated. Alcohol septal ablation (ASA) is performed by balloon angioplasty, with injection of alcohol into the enlarged area to create toxic necrosis. ASA induces shrinkage similar to myectomy. In appropriate cases, it abolishes the huge pressure gradient (Figure 1), which immediately induces liberation of enzymes (Figure 2). These changes are followed by LVOT-area enlargement over time accompanied by improved NYHA class.
|
Figure 1. Septal Ablation for HOCM.
【Click to enlarge】 |
|
|
|
Figure 2. Septal Ablation for HOCM.
【Click to enlarge】 |
|
|
|
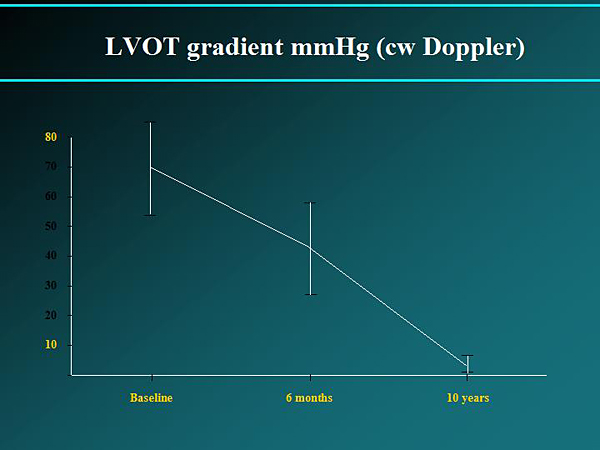
Figure 3. LVOT gradient mmHg (cw Doppler).
【Click to enlarge】 |
|
|
|
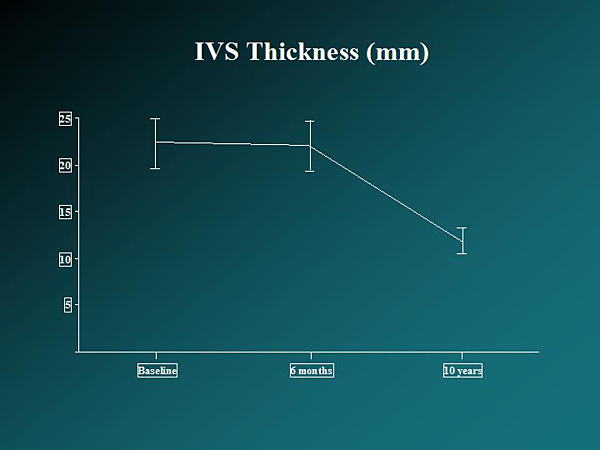
Figure 4. IVS Thickness.
【Click to enlarge】 |
|
|
|
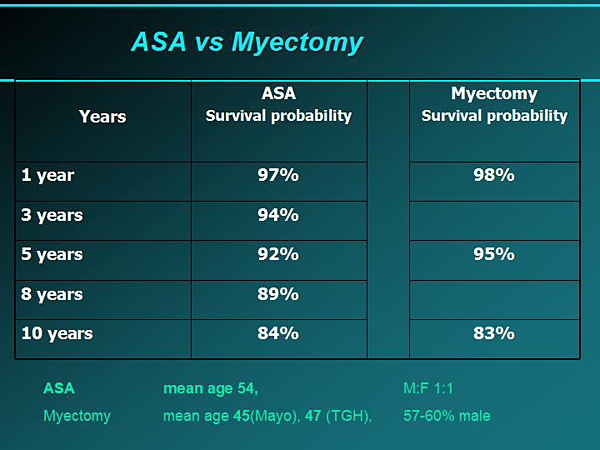
Figure 5. ASA vs Myectomy.
【Click to enlarge】 |
|
|
Eligibility criteria for ASA are symptomatic HOCM with systolic anterior movement of the mitral valve, septum thickness >18 mm, resting gradient >30 mmHg, and provoked gradient >60 mmHg. ASA is minimally invasive, less expensive than surgery, and can be performed more than once. Disadvantages are variations in the amount of offending myocardium removed, anatomical constraints, increased AV blocks, and possible arrhythmogenic scarring. Alcohol potentially can contaminate the conduction system, and is associated with an AV block rate of up to 15% and possible late AV blocks, ventricular fibrillation (VF), and sudden cardiac death.
A study investigating coil septal embolization involved placing coils into the first and second septal branches. Coil septal embolization was successful in 100% of patients, with use of 3.7 ± 1.8 coils per patient. Embolization induced a limited MI. The NYHA class and peak O2 consumption improved. There was one treatment failure with no improvement of LVOTG. No ventricular arrhythmias or AV blocks occurred. Bundle branch block occurred in 10% of patients. The procedure was associated with significantly improved symptoms and significantly reduced LVOTG and IVS thickness. A limitation is reduced efficacy versus alcohol ablation due to the unpredictable degree of collateral supply.
Microsphere embolization has been investigated as a way to avoid AV block and the need for pacemakers. The procedure produces significantly improved resting and provoked LVOTG (p <0.001). Further studies are needed to determine the safety and efficacy of this procedure.
ASA has a proven record of safety and efficacy over up to 16 years. Follow-up of the first ASA 11 patients at the Brompton in 1995 showed reduced LVOTG (Figure 3) and IVS thickness (Figure 4). LVEDD and LVESD were increased. Follow-up showed that there were no early deaths, 2 sudden deaths at 8 and 9 years, 1 metastatic pancreas carcinoma, gradient reduction maintained over >10 years, and long-term symptom reduction in all patients.
The large early ASA series at Baylor (N=213) and the Mayo Clinic (N=138) demonstrated long-term reductions in LVEF (Baylor, from 75% to 63%) and gradient (Mayo, from 80 mmHg to 10 mmHg), and 15% (Baylor) and 20.4% (Mayo) need for permanent pacemaker. The later Baylor-Charleston series (N=619) reported preserved LVEF, peak CK elevation of 1221 ± 716, and 8-10% need for pacemakers. For up to 10 years follow-up: Most patients’ angina and dyspnea scores improved from class 2 or 3 to class 1 and were maintained; septal thickness, LVOTG, and NYHA score decreased; treadmill time went up and remained increased; and LVEF decreased from 68 to about 62 over time. Event-free survival was 88% at 1 year and 80% at 5 years. Pacemaker was needed for AV block in 28% of the initial 50 patients, then decreased to 6.5% in the subsequent 579 patients. Death occurred in 12% of patients <50 years and 53% of patients >70 years, with 6 procedure-related deaths. The procedure was successful in 98.4% (N=629) of patients. Repeat ASA was done in 14% (N=81) of patients. Five patients had residual gradients and underwent subsequent myectomy.
Comparison of ASA versus myectomy shows similar survival probabilities (Figure 5). A meta-analysis of 42 ASA studies led to the conclusion that ASA results in favorable acute and intermediate-term clinical and echocardiographic outcomes. A randomized controlled trial is needed to compare ASA and myectomy. A recent update (Mayo, 2010) concluded that ASA shows promise in the treatment of HOCM; however, the caveat is increased conduction abnormalities and higher post-intervention LVOTG. The choice of treatment strategy should be made after a thorough discussion of the procedures with the patient. Dr. Sigwart concluded that ASA is effective for HOCM in the short- and long-term, relieving symptoms and gradients, and does not produce unwanted LV dilatation. ASA is more effective than DDD pacing and as effective as myectomy in appropriate cases.
|