Adnan Kastrati, MD, Klinikum rechts der Isar Technische Universitat, discussed the randomized clinical trials (RCTs) conducted by the ISAR Group. ISAResearch has completed 46 RCTs and has 10 ongoing RCTS, with more than 45,000 patients enrolled. The main focus areas of ISAR’s trials are adjunct peri-PCI antithrombotic therapy, optimal strategy in acute coronary syndrome (ACS), and improvement of stent technology.
The first ISAR trial (1996) reported significant reductions in bleeding events and ischemic cardiac complications in patients randomized to antiplatelet (N=257) versus anticoagulant (N=260) therapy followed by stenting. A 2001 study found that with ticlopidine therapy, the thrombotic event rate within 48 hours after stenting was 55%. A study comparing ticlopidine 500 mg with clopidogrel 300 mg and 600 mg showed that the full drug effect was achieved with clopidogrel 600 mg within 1-2 hours of giving a full loading dose. The ISAR-CHOICE trial found that plasma concentrations of clopidogrel and its active metabolite were significantly higher with the 600 and 900 mg doses versus the 300 mg dose. Lower values for platelet aggregation were observed with the 600 mg (p=0.01) and 900 mg (p=0.004) doses versus the 300 mg dose. The ISAR-CHOICE 2 trial showed that platelet inhibition was signficantly greater with 150 mg versus 75 mg maintenance clopidogrel (p<0.001). The CURRENT/OASIS 7 trial reported decreased risk of cardiovascular death, MI, and stroke with clopidogrel 600 mg loading dose followed by 150 mg maintenance versus 300 mg loading dose and 75 mg maintenance (HR=0.85, p=0.036).
ISAR-REACT and ISAR-SWEET found no benefit in the rate of cardiovascular events with abciximab versus placebo in elective PCI patients pretreated with 600 mg clopidogrel. Similar results were reported for bivalirudin versus unfractionated heparin (UFH) with respect to death, MI, urgent target vessel revascularization (UTVR), and major bleeding in ISAR-REACT 3. Separate analysis of bleeding events showed that bivalirudin versus UFH was associated with significantly fewer major (p=0.008) and minor (p=0.0001) bleeding events. Another study reported that all subgroups with reduced risk of bleeding with bivalirudin had an increased risk of MI (p=0.02). Bivalirudin therapy should be limited to patients with a high risk of bleeding and low risk of MI. Multivariate analysis of 5,384 ISAR patients showed that bleeding (HR=2.96) and MI (HR=2.29) were the most significant risk factors for one-year mortality.
|
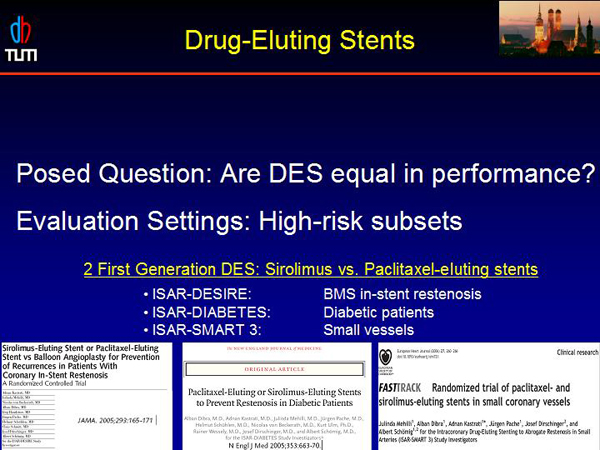
Figure 1. Drug-Eluting Stents.
【Click to enlarge】 |
|
|
|
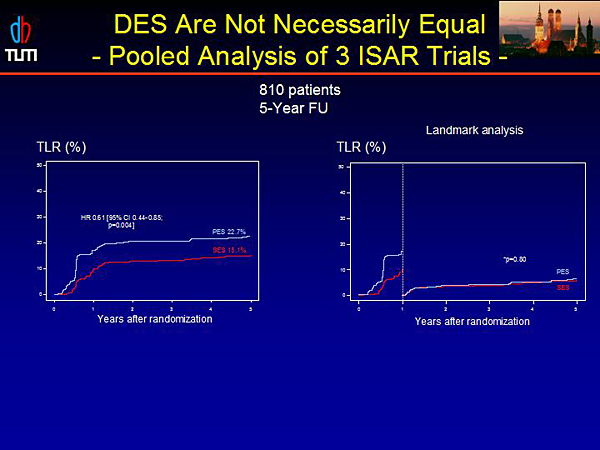
Figure 2. DES are not Necessarily Equal – Pooled Analysis of 3 ISAR Trials.
【Click to enlarge】 |
|
|
|
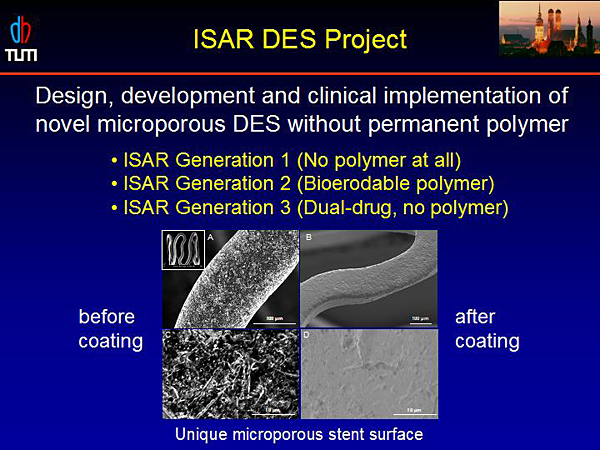
Figure 3. ISAR DES Project.
【Click to enlarge】 |
|
|
|
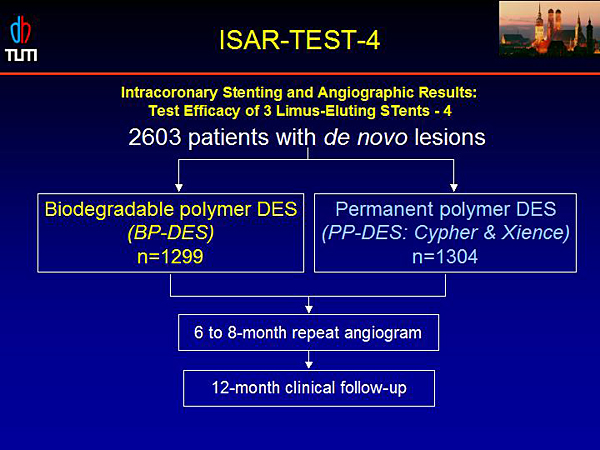
Figure 4. ISAR-TEST-4.
【Click to enlarge】 |
|
|
|
Figure 5. Duration of DAPT – ISAR-SAFE Trial.
【Click to enlarge】 |
|
|
ISAR-REACT2 reported a signficantly reduced rate of death/MI/UTVR in ACS PCI patients receiving abciximab (8.9%) versus placebo (11.9%) (RR=0.75). Most of the benefit was seen in troponin-positive (RR=0.71) versus troponin-negative (RR=0.99) patients. The Brave 3 trial in STEMI patients found no difference between abciximab and placebo in final infarct size or clinical outcomes.
ISAR-COOL compared delayed PCI (72-120 hours) versus early PCI (<6 hours) in ACS patients receiving antithrombotic pretreatment. The early PCI group had significantly reduced incidence of death and MI versus the delayed PCI group (p=0.04). The increase in MI/death in the delayed group occurred before catheterization (p=0.002); after catheterization the number of events was the same in both groups.
A study evaluating myocardial salvage with reperfusion therapy in AMI patients reported significantly increased survival in high salvage patients versus low salvage patients (p=0.001). The BRAVE trial reported no advantage to facilitated PCI (early, planned PCI after pharmacologic treatment to open the infarct-related artery) with respect to final infarct size and clinical outcomes. The ASSENT and FINESSE studies confirmed these results.
The BRAVE 2 trial found that PCI performed in asymptomatic patients >12 hours after STEMI onset resulted in reduced infarct size versus medical therapy (p=0.0002). After 4 years, the risk of death was lower in patients treated with PCI (adjusted HR=0.55, p=0.040).
The results of the ISAR-STEREO trials on the impact of stent strut thickness on restenosis led to the current dominant use of thin struts for coronary stents. Three ISAR trials evaluated the performance of drug-eluting stents (DES) (Figure 1). Pooled analysis of the trials demonstrated a 39% lower risk of target lesion revascularization (TLR) in patients receiving sirolimus-eluting stents (SES) versus paclitaxel-eluting stents (PES) (p=0.004) (Figure 2). A meta-analysis of 17 trials confirmed these results, showing the superiority of SES versus PES in reducing risk of reintervention (HR=0.74) and stent thrombosis (HR=0.66).
The ISAR DES project aimed to develop a novel microporous DES without permanent polymer (Figure 3). Four ISAR-TEST trials evaluated polymer- and nonpolymer-based DES with different drugs. ISAR-TEST4 is evaluating the efficacy of 3 limus-eluting stents (Figure 4). One-year results showed no difference between the BP-DES and PP-DES in incidence of cardiac death, MI, or TLR.
The optimal length of clopidogrel therapy after DES is an open question. The ISAR-SAFE trial is comparing 6-month versus 12-month therapy with clopidogrel in 6,000 DES patients (Figure 5). The primary endpoint is a composite of death, MI, stent thrombosis, stroke, and major bleeding at 15 months. The trial design was published in the American Heart Journal in 2009.
|