Arthur J. Moss, MD, University of Rochester Medical Center, discussed the results of the MADIT trials on reducing or eliminating sudden cardiac death (SCD) and preventing heart failure in high-risk patients. The MADIT-I trial (1996) enrolled 196 patients with a history of MI, ejection fraction (EF) ≤0.30, an episode of non-sustained ventricular tachycardia (NSVT), and a positive electrophysiological study. The patients were randomized to receive an implantable cardiac defibrillator (ICD) or best conventional therapy. There was a significant reduction in mortality in the ICD versus conventional therapy group (HR=0.46, p=0.009). The benefit of ICD therapy occurred primarily in patients with heart failure (HF) (p=0.01), while patients without HF did not have a significant benefit.
The MADIT-II trial (2002) enrolled 1,232 patients with a history of MI and EF ≤30% to receive an ICD or conventional therapy. The ICD group had a significant reduction in mortality versus the conventional therapy group (HR=0.69, p=0.016). Hospitalization for HF after discharge was a risk factor for subsequent appropriate ICD therapy (HR=2.5, p=0.001) but MI/unstable angina (UA) was not a significant risk factor. The one-year mortality rates were: 5% in patients whose ICD did not discharge (SCD 2%, HF 3%); 15% after first ICD therapy for VT (SCD 7%, HF 8%); and 20% after first ICD therapy for ventricular fibrillation (VF) (SCD 4%, HF 16%).
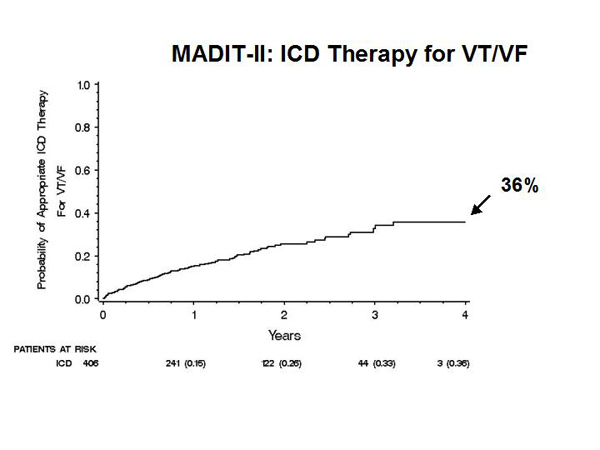
In the MADIT-1 and MADIT-II trials, life-prolonging ICD therapy appeared to transform a risk of SCD into a later risk for HF. In MADIT-II, only 36% of patients with an ICD had ICD therapy for VT or VF over 4 years (Figure 1). The low percentage of patients who used their ICD led to a clinical risk stratification approach for patient selection. A very high risk (VHR) group with BUN >50 mg/dL was identified. A risk score was developed using simple clinical factors in the conventional therapy group.
|
Figure 1. MADIT-II ICD Therapy for VT/VF.
【Click to enlarge】 |
|
|
|
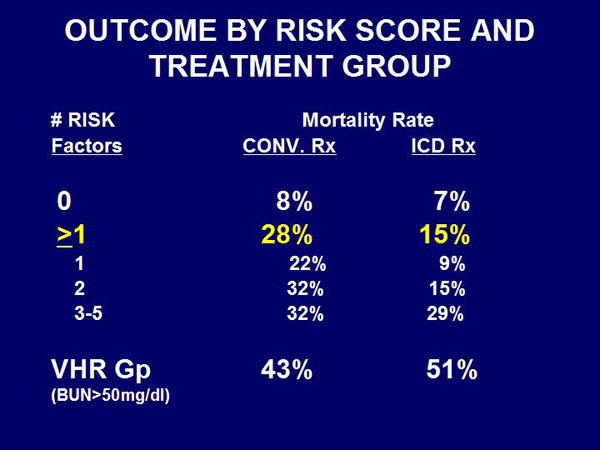
Figure 2. Outcome by Risk Score and Treatment Group.
【Click to enlarge】 |
|
|
|
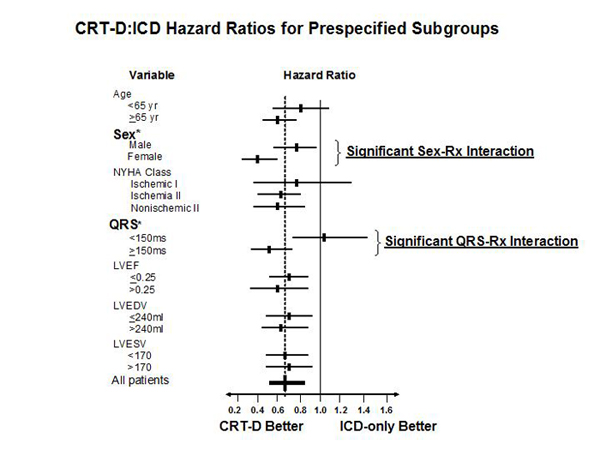
Figure 3. CRT-D:ICD Hazard Ratios for Prespecified Subgroups.
【Click to enlarge】 |
|
|
|
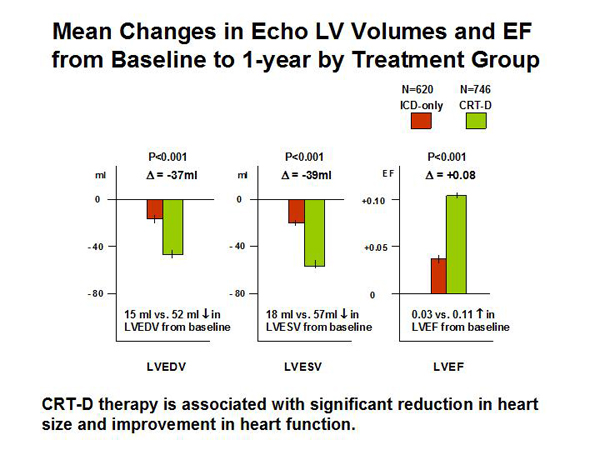
Figure 4. Mean Changes in Echo LV Volumes and EF from Baseline to 1-Year by Treatment Group
【Click to enlarge】 |
|
|
|
Figure 5. MADIT-IV: MADID-RIT
【Click to enlarge】 |
|
|
Risk factors for all-cause mortality in the conventional therapy group were NYHA >II (HR=1.87, p=0.004), atrial fibrillation (HR=1.87, p=0.03), QRS >120 ms (HR=1.65, p=0.02), age >70 years (HR=1.57, p=0.04), and BUN >26 to <50 mg/dL (HR=1.56, p=0.04). The mortality rate for patients with ≥1 risk factor was 28% in the conventional therapy group versus 15% in the ICD group (Figure 2). Mortality in the VHR group was 43% in the conventional therapy group versus 51% in the ICD group. About one-third of patients (0 risks and VHR) received no benefit from ICD therapy. The patients with ≥1 risk factor received the greatest benefit from an ICD (HR=0.45). The benefit from ICD therapy continued over time, with 0.6 life-years saved over 8 years (HR=0.63, p <0.001).
The aim of the MADIT-CRT trial (2009) was to reduce the occurrence of heart failure in patients resuscitated with a defibrillator by using cardiac resynchronization therapy (CRT). Patients (N=1,820) with NYHA I/II cardiomyopathy, decreased EF, and wide QRS were randomized to receive an ICD only or an ICD with CRT (CRT-D). The death/HF rate was 25.3% in the ICD group versus 17.2% in the CRT-D group (HR=0.66, p=0.001). The HF rate was 22.8% in the ICD group versus 13.9% in the CRT-D group (HR=0.59, p<0.001). There was little reduction in death (HR=0.89, p=0.72) but the investigators believe the reduction in HF will result in a reduction in mortality over time. Subgroup analysis demonstrated that most subgroups derived benefit from CRT-D versus ICD, except for patients with narrow QRS (Figure 3). Women had a significantly greater benefit from CRT-D therapy than men. Echocardiogram demonstrated significantly reduced left ventricular end-diastolic volume (LVEDV) (p <0.001) and LV end-systolic volume (LVESV) (p <0.001) and increased EF (p <0.001) in the CRT-D group versus the ICD-only group (Figure 4).
The objective of the ongoing MADIT-RIT trial is to reduce inappropriate ICD therapy in a planned population of 1,500 patients with an ICD for primary prevention only (Figure 5). The patients are being randomized to three arms: Standard ICD therapy, high-rate cutoff ICD therapy, and long delay ICD therapy. The primary endpoint is first inappropriate ATP or shock therapy at a minimum follow-up of 12 months.
Dr. Moss concluded with a summary of the current ACC/AHA Guidelines. The 2005 Guidelines recommend CRT for patients with sinus rhythm, widened QRS interval (≥120 ms), severe LV dysfunction (EF ≤0.35), and severe HF (NYHA class III/IV) despite optimal medical therapy. The 2008 Guidelines recommend ICD in: Ischemic heart disease (IHD) (NYHA II/III) patients with EF ≤35% at least 40 days post-MI, who are receiving chronic optimal medical therapy and who have reasonable expectation of survival with good functional status for >1 year; IHD (NYHA I) patients with EF ≤30% at least 40 days post-MI, who are receiving chronic optimal medical therapy and who have reasonable expectation of survival with good functional status for >1 year; and Non-ischemic dilated cardiomyopathy (NIDCM) (NYHA II/III) patients with EF ≤35% for >3 months who are receiving chronic optimal medical therapy and who have reasonable expectation of survival with good functional status for >1 year.
|