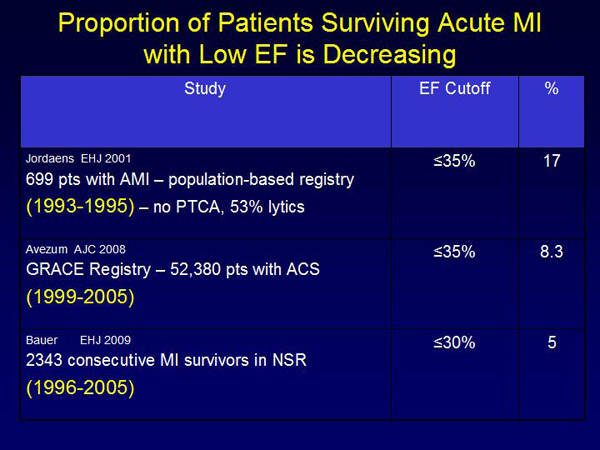
Alfred E. Buxton, MD, Alpert Medical School of Brown University, reviewed studies on risk factors for sudden cardiac death (SCD). Although LVEF is a good predictor of total mortality after MI, population-based studies show that patients with low LVEF account for only half of those with SCD. Among patients who survive acute MI there has been a decline in the percentage with low LVEF, because of reperfusion therapy (Figure 1). In the GUSTO trial, 12% of acute MI survivors had LVEF ≤40%. A meta-analysis showed that LVEF does not predict the cause of death after MI.
|
Figure 1. Proportion of Patients Surviving Acute MI with Low EF is Decreasing.
【Click to enlarge】 |
|
|
|
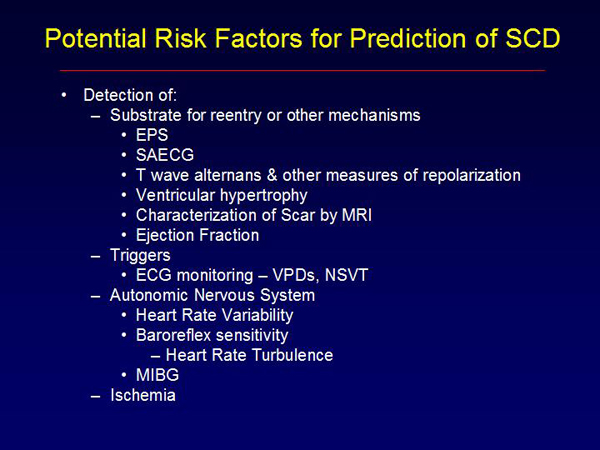
Figure 2. Potential Risk Factors for Prediction of SCD.
【Click to enlarge】 |
|
|
|
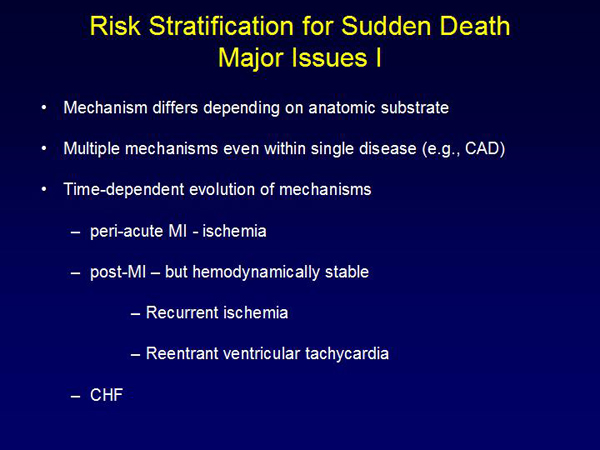
Figure 3. Risk Stratification for Sudden Death: Major Issues
【Click to enlarge】 |
|
|
|
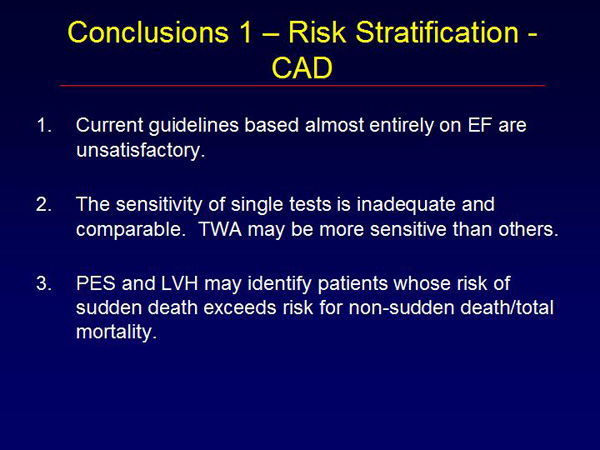
Figure 4. Conclusions 1 – Risk Stratification CAD.
【Click to enlarge】 |
|
|
|
Figure 5. Conclusions 2 – Risk Stratification.
【Click to enlarge】 |
|
|
In the MADIT II study post-MI patients with BUN ≥50 mg/dL and/or creatinine ≥2.5 mg/dL had no improvement in all-cause mortality with defibrillator therapy versus pharmacologic therapy. After eliminating patients with severe renal dysfunction, multivariate analysis identified NYHA Class >2 (HR=1.87, p=0.004), atrial fibrillation (HR=1.87, p=0.034), QRS >120 ms (HR=1.65, p=0.020), age >70 years (HR=1.57, p=0.042), and BUN 27-49 (HR=1.56, p=0.048) as risk factors for mortality. Patients with 1 or 2 of these factors had a significant survival benefit with ICD therapy. Patients with none and those with ≥3 risk factors had no survival benefit. Altogether, 46% of patients derived no survival benefit from an ICD. Thus, using current risk factors to guide ICD use, most post-MI patients who die suddenly are being missed.
Figures 2 and 3 list potential risk factors for SCD and major issues associated with them. In the ATRAMI study, patients with LVEF <35 and baroreflex sensitivity (BRS) <3 had markedly lower event-free survival (EFS) than those with LVEF <35 and BRS ≥3, LVEF ≥35 and BRS <3, or LVEF ≥35 and BRS ≥3 (p <0.001). Other studies have shown: Higher arrhythmic event rates in patients with T-wave alternans (TWA) and late potentials (LP) versus those with one or neither factor (p<0.0001); in patients with LVEF >40% post-MI, those with TWA had lower EFS versus patients without TWA (p <0.001); in post-MI patients with LVEF >35%, those with BRS <3 ms/mmHg had increased cardiovascular deaths versus patients with BRS ≥3 ms/mmHg (p <0.0001).
Multiple studies have demonstrated that sensitivity of single risk stratification tests is below 80%. MUSTT, the only prospective trial to study test sensitivity, using electrophysiologic testing (EPS) found that 18% of patients with inducible ventricular tachycardia (VT) had cardiac arrest versus 12% of those without inducible VT (p <0.001). Patients with inducible VT treated with ICD had lower risk for cardiac death (p <0.001).
Dr. Buxton’s conclusions are listed in Figures 4 and 5. “None of the studies address the population in which cardiac arrest is the initial manifestation of heart disease—a far greater challenge,” he concluded. |