|
|
APSC-JCS Joint Symposium |
| |
| Detection of Unstable Plaques and Assessment of Responses to Treatment -Advance in Imaging- |
|
| |
|
| Detection of Coronary Artery Plaques with Magnetic Resonance Imaging |
| Tae-Hwan Lim, MD, PhD, FAHA |
| University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea |
| |
Dr. Tae-Hwan Lim, Asan Medical Center, Seoul, Korea, discussed the evaluation of coronary plaque morphology and biology using magnetic resonance imaging (MRI). Conventional coronary MRI has limited spatial resolution and data sampling. The development of coronary MRI using 2D free breathing with T2 weighted (T2W) total spin-echo (TSE) improves resolution, producing higher contrast images.
In 2002, Kim et al developed a 3D-spiral readout acquisition technique with free breathing, double inversion recovery (IR), fat saturation, and very short repetition time (TR) and echo time (TE), to produce clear, high contrast images of coronary vessels. Using this technique, the investigators demonstrated significantly increased average wall thickness in patients with non-significant coronary artery disease (CAD) compared with healthy subjects (p<0.01). There was no difference in lumen diameter, indicating the presence of remodeling.
The MESA trial used double IR, navigator gated, fat suppression, and T2 TSE MRI with free breathing to clearly image positive remodeling. In both men and women, the vessel size was normal, the mean vessel wall thickness was increased, and the total vessel area was increased, demonstrating positive remodeling.
|
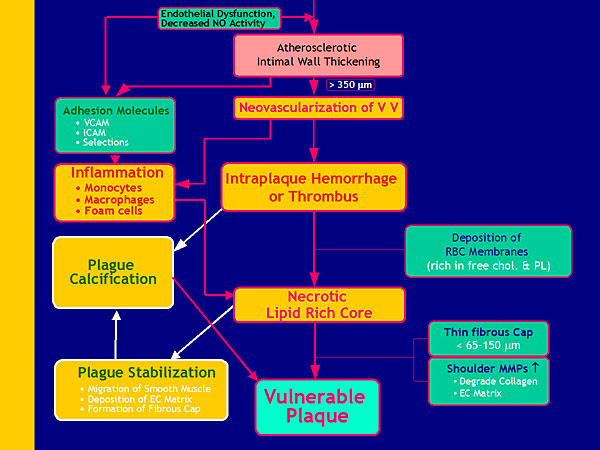
Figure 1. Development of vulnerable plaque.
【Click to enlarge】 |
|
|
In a recent study using micro CT, abundant vaso vasorum (adventitial blood vessels) were observed in areas of rich plaque, especially on the external portion of the vessels. Growth and extension of the vaso vasorum into the intima occurs in response to tissue hypoxia when the intima thickens beyond the diffusion limit of oxygen and nutrients (Figure 1). In another study, CT revealed a low density plaque with positive remodeling in a patient’s right coronary artery. MRI of the same vessel showed linear hyperintense lesions corresponding to the plaque. One year later the patient had total occlusion necessitating PCI; massive ultrasound attenuation was confirmed by IVUS. This and similar results in other patients show that hyperintense coronary plaques are related to positive remodeling, ultrasound attenuation, lower Hounsfield units, spotty calcifications, and transient slow flow after PCI.
Using contrast enhanced 3D T1W MRI with IR and turbo field-echo (TFE), Yeon et al observed calcified plaques in the LAD and circumflex artery that were not detected with CT, MR angiography, or non-enhanced MR. This finding shows that coronary plaque formation and vulnerability is not localized but is a diffuse phenomenon. Strong enhancement was observed in 36% of calcified plaques and 53% of patients with >20% stenosis.
|
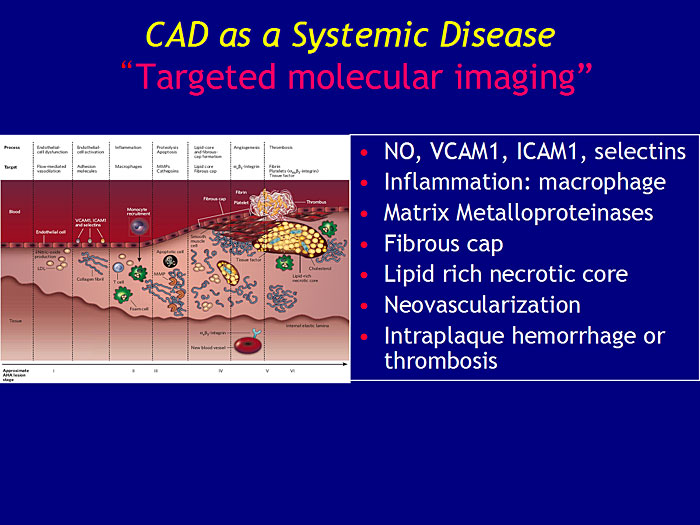
Figure 2. CAD as a Systemic Disease.
【Click to enlarge】 |
|
|
These studies show that in cases with diffuse enhancement, hemorrhage, or a lipid-rich core, the disease is not localized (Figure 2). Dr. Lim concluded that targeted molecular MR imaging is needed for further understanding of plaque morphology and biology of CAD as a systemic disease. |
| |
| Page Top |
|
| |
|
| Role of CT in Detection of Unstable Plaques and Assessment of Response to Treatment |
| Kui-Hian Sim |
| Sarawak General Hospital and University Malaysia Sarawak, Malaysia |
| |
|
Figure 1. Coronary angiography of acute coronary syndrome
【Click to enlarge】 |
|
|
|
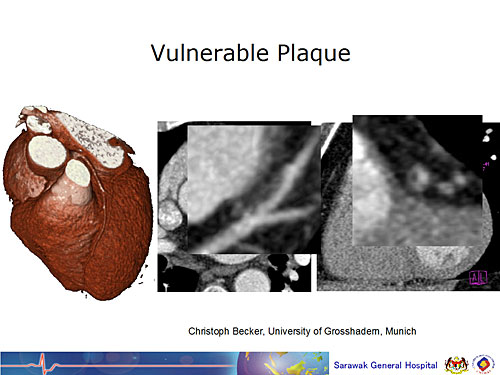
Figure 2. CT detection of vulnerable plaque at first visit
【Click to enlarge】 |
|
|
Dr. Kui-Hian Sim, University of Malaysia, Sarawak, reviewed recent studies of cardiac computed tomography (CT) for detecting unstable plaque. Coronary angiogram has been the gold standard for detecting plaque, even though recent evidence demonstrates that unstable plaque can be detected earlier with cardiac CT (Figures 1 and 2).
In 2006, Sim’s group presented results of a study in which they used CT with vessel density ratio (VDR), a novel method to evaluate plaque. VDR is the ratio of density (contrast attenuation) of the whole vessel segment to the density (attenuation) of the aortic root. Using this technique to evaluate 188 lesions in 64 patients, the investigators were able to distinguish between stable angina, unstable angina/NSTEMI, and STEMI. The technique also distinguished between non-ACS (stable angina) and ACS lesions. Among the ACS lesions, it differentiated between culprit and non-culprit lesions, allowing determination of which should undergo angioplasty. The results were confirmed by Hoffman et al who identified differences in lesion morphology and plaque composition between ACS culprit lesions and ACS stable lesions/stable angina using CT.
In a study comparing 64-slice CT with intravascular ultrasound (IVUS), CT demonstrated 90% accuracy in detecting any plaque. In 94% of sections, atherosclerotic lesions were excluded correctly by CT. However, CT systematically underestimated noncalcified and mixed plaque volume and overestimated calcified plaque volume. Another study showed that, although plaque volume is not accurately calculated, composition can be accurately determined. The presence of positive remodeling, noncalcified plaque <30 Hounsfield Units (HU), and spotty calcification had a high positive predictive value for the presence of ACS lesions. Absence of all three had a high negative predictive value.
A study of reproducibility of plaque volume and composition quantification by coronary CT angiography (CCTA) showed that the most accurate measure is the percentage of plaque composition rather than plaque volume, especially in smaller plaques. Based on the results of these studies, CCTA quantification of total plaque volume is accurate with large plaques, but accuracy declines with decreasing plaque size. Mixed plaques are likely to be underestimated by CCTA, while calcified plaques are likely to be overestimated.
Studies of CT in ACS are also evaluating its use for assessing myocardial perfusion and ventricular function. Looking to the future, molecular techniques in addition to CT imaging need to be studied for diagnosis of vulnerable plaque. To achieve the ultimate goal of preventing coronary events, methods for detecting vulnerable plaque need to be evidence based, while outcomes assessment needs to be economics based. In conclusion, CT for detecting unstable plaques and assessing response to treatment has high spatial resolution, temperature resolution, penetration, and clinical use, but sensitivity and specificity are low.
|
| |
| Page Top |
|
| |
|
| Molecular Imaging of Plaque Inflammation |
| Nobuhiro Tahara |
| Kurume University School of Medicine |
| |
|
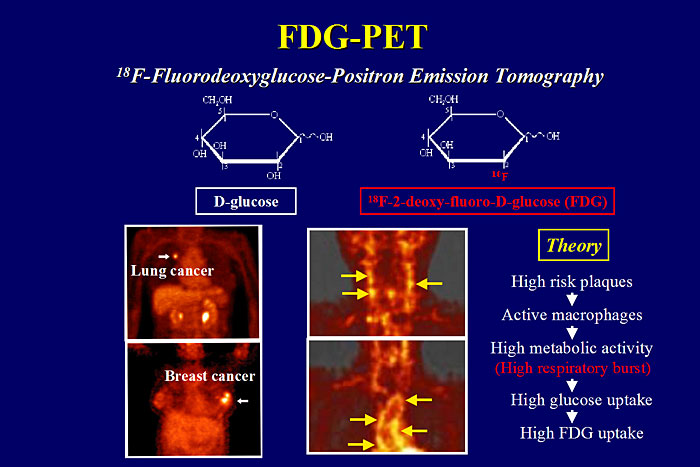
Figure 1. FDG-PET
【Click to enlarge】 |
|
|
Morphologic features of atherosclerotic plaque have been visualized using ultrasound, CT angiography, MRI, intravascular ultrasound, and optical coherence tomography. However, these imaging techniques do not reveal the extent of plaque inflammation. Dr. Nobuhiro Tahara, Kurume University School of Medicine, reviewed studies of PET imaging as a noninvasive technique for quantifying atherosclerotic plaque inflammation.
18F-fluorodeoxyglucose-positron emission tomography (FDG-PET) has been widely used for imaging malignant tumors based on increased uptake of FDG, a glucose analogue. Enhanced FDG accumulation is also observed in neutrophils and macrophages in inflammatory lesions (Figure 1). The Cambridge team reported that FDG-PET detected carotid atherosclerotic plaque in patients with recent transient ischemic attack. Histologic analysis revealed that FDG accumulation primarily corresponded to the macrophage-rich region of the plaque.
|
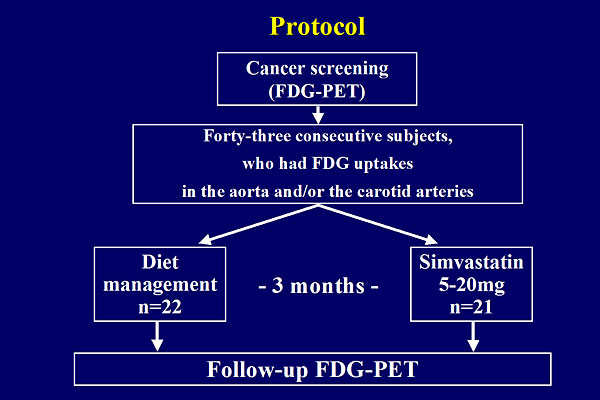
Figure 2. Statin Study Protocol
【Click to enlarge】 |
|
|
|
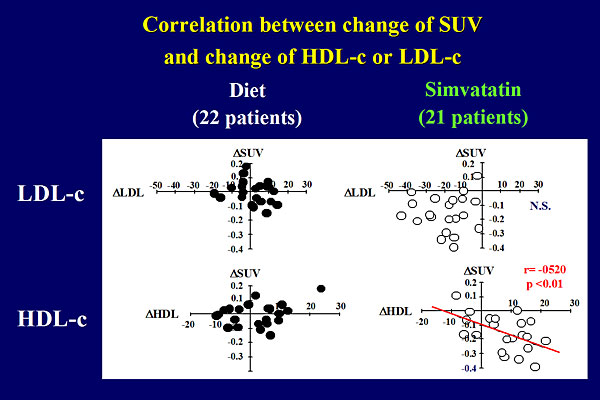
Figure 3. Correlation between change of SUV and change of HDL-c or LDL-c
【Click to enlarge】 |
|
|
Dr. Tahara’s group used FDG-PET to evaluate the extent of vascular inflammation in atherosclerotic plaques in 100 consecutive patients who underwent carotid artery ultrasound screening. Ultrasound detected carotid atherosclerosis in 40% of the patients. FDG-PET demonstrated inflammation in 29% of the plaques. Next, the relationship between vascular inflammation evaluated by FDG-PET and metabolic risk factors was assessed in 216 patients. Multiple stepwise regression analysis showed that vascular inflammation was associated with waist circumference (p<0.001), antihypertensive therapy (p<0.001), carotid thickness (p<0.001), HDL-cholesterol (p<0.01), insulin resistance (p<0.05), and CRP (p<0.05). Age- and gender-adjusted FDG levels were significantly higher as the number of metabolic syndrome risk factors increased (p<0.0001).
Dr. Tahara examined the effects of statins on plaque inflammation in 43 patients randomized to simvastatin or dietary modification (Figure 2). After 3 months, FDG-PET scans showed a significant reduction in plaque inflammation in the statin group (p<0.01) but not in the diet group. The extent of FDG uptake did not correlate with the statin-induced reduction in LDL-cholesterol but did positively correlate with increased HDL-cholesterol levels (p<0.01) (Figure 3).
|
Figure 4. Pioglitazone study protocol
【Click to enlarge】 |
|
|
|
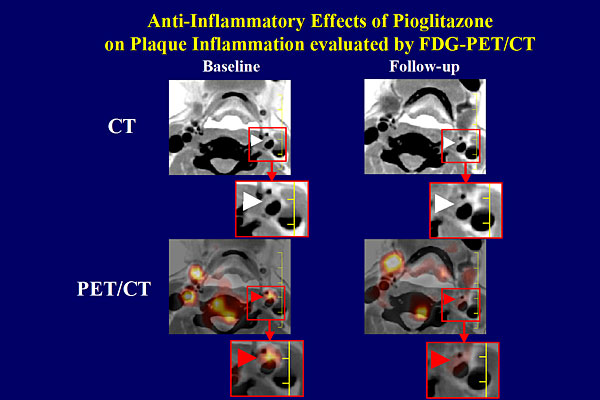
Figure 5. Anti-inflammatory effects of pioglitazone on plaque inflammation evaluated by FDG-PET/CT.
【Click to enlarge】 |
|
|
The PROactive study showed that pioglitazone dramatically reduces the incidence of stroke in diabetic patients (p=0.009). Dr. Tahara examined the effects of pioglitazone on plaque inflammation using FDG-PET in 32 patients randomized to glimepiride or pioglitazone (Figure 4). After 4 months of treatment, FDG uptake was reduced in the pioglitazone group (Figure 5). Pioglizatone attenuated inflammation but glimepiride did not (p<0.01). This finding suggests that pioglitazone has anti-inflammatory effects on carotid plaque, which may be a mechanism for the stroke reduction observed with pioglitazone.
A study of coronary artery FDG-PET demonstrated FDG uptake in the left main coronary artery and aortic root, as well as at the site of a coronary stent in a patient who had undergone primary PCI. This study suggests that PET and CT may be useful tools for identifying inflammatory coronary lesions.
|
| |
| Page Top |
|
| |
| |
|
|