Critical Leg Ischemia (CLI) results in substantial morbidity and mortality, with 10-40% of patients requiring amputation within one year and a 20% one-year mortality rate. Current therapeutic options are limited to revascularization, conservative wound management, and amputation. Researchers at Osaka University have identified hepatocyte growth factor (HGF) as a potent stimulator of angiogenesis. Dr. Ryuichi Morishita, Osaka University Graduate School of Medicine, described clinical studies of HGF in patients with limb ischemia.
In the first human study of HGF (JN-100-Osaka, 2004), 22 patients with peripheral artery disease (PAD) and Buerger’s disease received intramuscular injections of HGF plasmid DNA. Improvement was observed in ulcer healing (63.6%), resting pain (61.5%), and ankle brachial pressure index (ABPI) (64.7%).
|
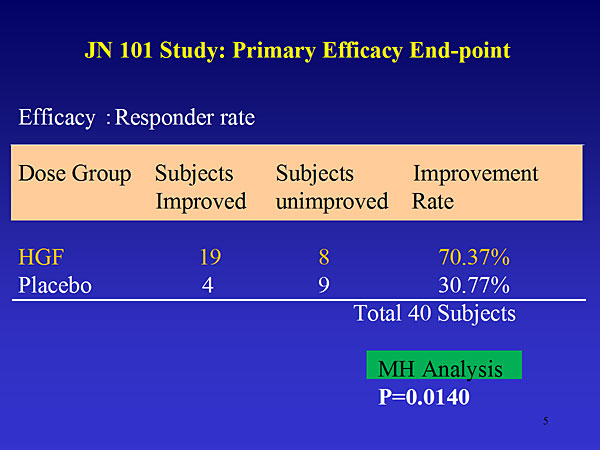
Figure 1. JN 101 Study: Primary Efficacy Endpoint.
【Click to enlarge】 |
|
|
A phase III study (JN-101) was conducted in Japanese patients with Fontaine III/IV PAD. The trial was designed to randomize 120 patients to HGF plasmid or placebo but was stopped at 40 patients because of the high efficacy of HGF. A total of 27 patients received HGF plasmid injections and 13 received placebo. The efficacy endpoints were change in rest pain and ulcer size. The improvement rate was 70.4% in HGF patients and 30.8% in placebo patients (p=0.0140) (Figure 1). After 12 weeks follow-up, ulcer size was reduced by 70% in the HGF group versus no improvement in the placebo group. HGF versus placebo also improved bodily pain (p=0.036) and mental health (p=0.023). Adverse events were evenly distributed between the HGF and placebo groups. Based on these studies, HGF gene therapy will be launched in 2010 in Japan.
|
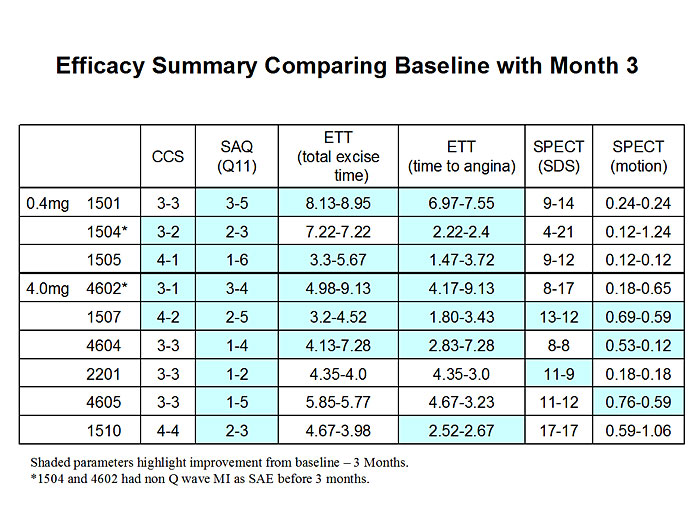
Figure 2. Efficacy Summary Comparing Baseline with Month 3.
【Click to enlarge】 |
|
|
|
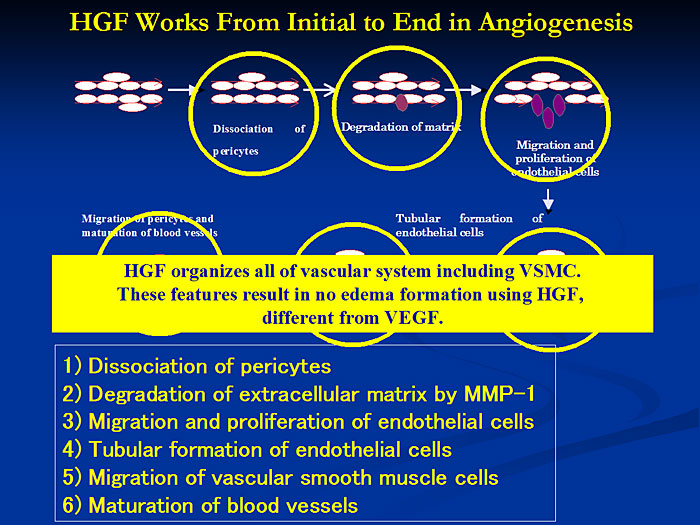
Figure 3. HGF Works from Initial to End in Angiogenesis.
【Click to enlarge】 |
|
|
|
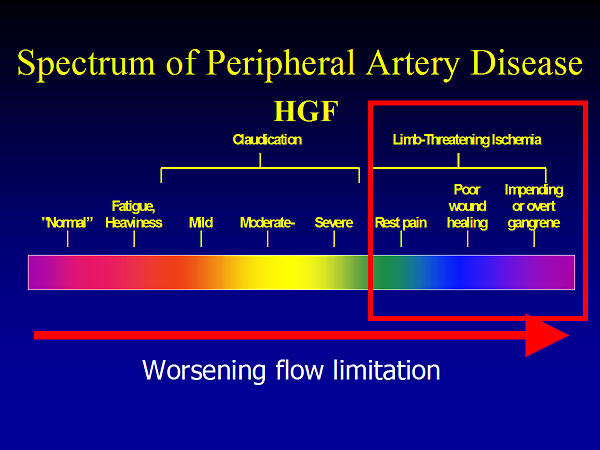
Figure 4. Spectrum of Peripheral Artery Disease
【Click to enlarge】 |
|
|
A phase II US study randomized patients with CLI to placebo (N=25), 0.4 mg HGF on days 0, 14, and 28 (N=25), 4 mg HGF on days 0 and 28 (N=25), and 4 mg HGF on days 0, 14, and 28 (N=25). The high-dose (4 mg x3) group had significant improvement in transcutaneous oxygen pressure (TcPO2) at 6 months (p=0.011).
In 2010, Dr. Morishita’s group started a phase III multinational study that plans to randomize CLI patients with no or poor options for revascularization to two sets of HGF or placebo injections. The group is also conducting a phase I study of intramyocardial injections of naked plasmid HGF DNA in patients with ischemic heart disease. Early results are shown in Figure 2.
In summary, HGF has primary control of angiogenesis. A single stimulation with HGF is enough to initiate and continue the process of angiogenesis from dissociation of pericytes to maturation of blood vessels (Figure 3). Dr. Morishita concluded that HGF might provide a new treatment for CLI patients with no or poor options for revascularization (Figure 4). |