Dr. David J. Callans, University of Pennsylvania School of Medicine, discussed the uses and techniques of epicardial ablation. Indications for epicardial ablation include Chagas disease, VT associated with dilated cardiomyopathy (DCM), post-MI (rarely), cardiac sarcoid, myocarditis, right ventricular (RV) cardiomyopathy, left ventricular (LV) non-compaction, and some forms of idiopathic VT.
Electrocardiographic (ECG) clues to the epicardial location of VT include appearance of a pseudo-delta wave or a precordial maximum deflection index ≥0.55. Callans has focused on the unexpected presence of Q waves in areas of the heart that are subtended by the ECG lead. If there is an epicardial focus on the basal inferior wall, a QS complex will be recorded in the inferior leads. In patients with VT just anterior to the aorta ECG shows a pattern break where V1 is positive, V2 is initially positive but has a deep S wave at the end of the QRS, and V3 is positive. This suggests that the VT is just underneath lead V2, which is anterior to the aorta.
|
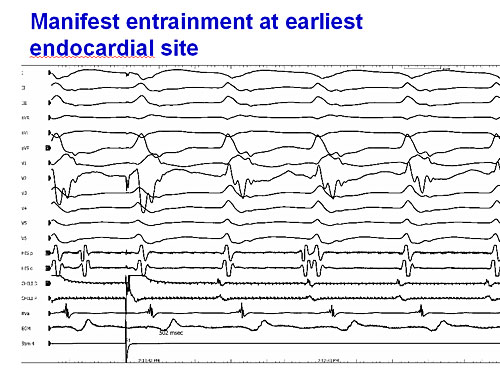
Figure 1. Manifest entrainment at earliest endocardial site
【Click to enlarge】 |
|
|
|
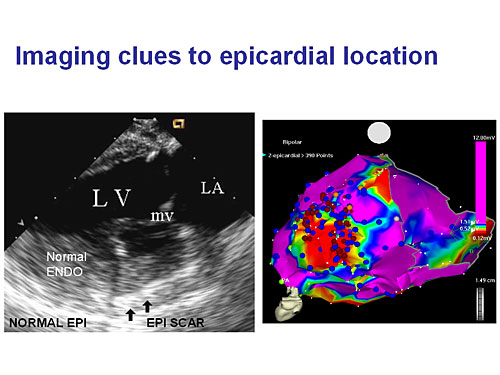
Figure 2. Imaging clues to epicardial location
【Click to enlarge】 |
|
|
Array mapping can also indicate VT located in the epicardium. This technique is important for locating VT for epicardial ablation in patients with DCM and RV cardiomyopathy. Additionally, when pacing is done at the site of earliest activation, manifest entrainment is seen, most easily noted in lead V2, suggesting an epicardial site (Figure 1).
MRI with delayed enhancement or intercardiac echocardiography can provide clues to epicardial location. In a patient with sarcoid and uniform VT, the epicardial surface looked normal but the subepicardium had a dense hyperechoic region that correlated with the scar observed on voltage mapping (Figure 2). Epicardial ablation was performed successfully in this patient.
The Cleveland Clinic did a study of epicardial ablation in 20 patients with idiopathic VT who failed endocardial ablation. The VT was mapped to epicardial sites in 9 of the patients and epicardial ablation was successful in 8 of these.
Unique problems associated with epicardial ablation include the need for general anesthesia and a potential for coronary artery occlusion, phrenic nerve damage, and persistent pericardial bleeding. Additionally, insulating epicardial fat can cause false low voltage areas on mapping and cause radio frequency ablation to fail. Both problems are ameliorated with cold ablation.
Dr. Callans concluded that epicardial origin of VT is a possible cause of failed endocardial ablation. The epicardial approach may be particularly important in idiopathic VT, VT in DCM, and VT in RV cardiomyopathy. |