|
|
||||||
|
|||||||
|
|||||||
|
|||
|
|||
Novel Inflammatory Markers in Acute Coronary SyndromeChristian W. HammKerckhoff Heart Center
|
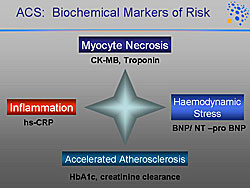
Established biochemical markers to assess patients with acute coronary syndrome (ACS) are shown in Figure 1. Inflammation plays a major role in the development of coronary artery disease (CAD).
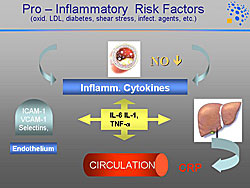
Pro-inflammatory risk factors include oxidated LDL, cholesterol, diabetes, sheer stress, and infectious agents, which result in the release of inflammatory cytokines (Figure 2). These stimulate in the liver the release of C-reactive protein (CRP), an acute phase reactant, which can be measured in the circulation.
|
|
CRP is the most widely investigated inflammatory marker. Ridker and colleagues have shown that in healthy subjects CRP is linked to the risk of myocardial infarction (MI). Further, the combination of CRP and cholesterol increases the predictive value.
The Reykjavik Prevention Study of primary prevention over 20 years reported in 2004 that CRP continues to have a predictive value. However, other risk factors, such as cholesterol, smoking, and blood pressure, have more pronounced predictive value.
In patients with ACS, it is well established that CRP is a very potent long-term marker for mortality. The FRISC study showed that CRP elevation is linked to elevated mortality; 20% at 4 years in patients with CRP > 10 mg/liter compared to about 8% in patients with CRP < 2 mg/liter. The PROVE-IT TIMI 22 trial showed that the combination of LDL cholesterol and CRP provided additive value; patients with the highest elevations of both had the highest event rate of recurrent MI or cardiac death and patients with the lowest levels of both had the lowest event rate.
Markers of local inflammation
Markers of transition from the early lesion to the vulnerable plaque are of the greatest interest. Thus, markers of local inflammatory processes are of interest, which indicate plaque de-stabilization and also provide some estimates of platelet activation. In contrast, CRP is a more global marker.
|

Markers of inflammation under investigation are shown in Figure 3. CRP is a systemic inflammatory marker, which probably has low specificity. Myeloperoxidase (MPO) is a marker of local inflammation investigated in stable angina pectoris and in ACS. Markers of vascular inflammation include the placental growth factor (PIGF) and pregnancy-associated plasma protein A (PAPP-A). Markers of thrombosis and inflammation include CD40 ligands. Markers of anti-inflammation, which have a protective role, include interleukin-10.
Myeloperoxidase
MPO is a marker of local inflammatory activity and is released from activated leukocytes. MPO also has pro-atherogenic properties. It supports the oxidation of LDL and therefore foam cell formation. It activates metalloproteinase-7 (MMP-7) and therefore produces erosion of plaques. MPO leads to the reduction of endothelial nitric oxide (NO), and therefore is involved in endothelial dysfunction.
Zhang and colleagues showed that plasma and leukocyte levels of MPO are higher in patients with CAD compared to patients without CAD. Hamm and colleagues showed in the CAPTURE study population that high MPO levels are associated with an adverse outcome. The hazard ratio for the risk of death and acute MI was 2.25 for patients with a high versus low MPO level over 6 months.
Combining risk factors increases the predictive value. Also in the CAPTURE population, they showed that patients with a low troponin T (TnT) and high MPO levels were at a higher risk for events (15.9%), while patients with low TnT and low MPO has a 2.0% risk, and the patients with high TnT and high MPO had a 24.6% risk. The combination of CRP and MPO showed that patients with a low CRP and a high MPO had the same risk as patients with high levels of CRP. Thus, MPO seems to play a special role to indicate the inflammatory process that occurs in the coronary arteries.
Soluble CD40 ligands
|
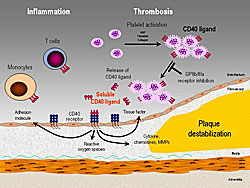
When platelets are activated, the CD40 ligands are expressed to the surface (Figure 4). These are cleaved into the circulation and the soluble CD40 (sCD40) ligands bind to the CD40 receptor on the endothelium and also bind to white blood cells. Therefore, sCD40 ligands establish the role between thrombosis and inflammation. sCD40 ligands bound to the endothelial receptor promote plaque de-stabilization by activating a number of different reactions in the endothelium.
Heeschen and colleagues showed that the level of sCD40 ligands is closely linked to the monocyte platelet aggregates and therefore platelet activation. Varo and colleagues showed patients with Type 1 and 2 diabetes have higher levels of sCD40 ligands compared to patients without diabetes. Schonbeck and colleagues first described the predictive value of sCD40 ligands; healthy women with sCD40 ligands in the 50th percentile had a 1.02 relative risk (RR), 75th percentile had a 1.35 RR, the 90th percentile a 1.92 RR, the 95th percentile 3.29 RR, and 99th percentile a 11.83 RR.
The levels of sCD40 ligands in different populations of CAD was described by Heeschen and colleagues. Patients with non-cardiac chest pain and stable angina have lower levels, below the threshold value of plasma soluble CD40 ligands (5 µg/L), and patients with unstable angina and non-ST segment elevation MI had higher levels (about 6-8 µg/L).
Hamm and colleagues showed in the CAPTURE study that patients with elevated sCD40 ligands, compared to lower levels, had a 3.4-fold higher risk of death and MI. Further, the combination of TnT and sCD40 ligands further increased the predictive value. Patients with a low TnT and low sCD40 had a 5.7% risk of death and MI compared to 14.9% for patients with a low TnT and a high sCD40 (p=0.012). Patients with a high TnT and a low sCD40 had a 10.5% risk of death and MI, compared to 24.3% for patients with a high TnT and a high sCD40 (p=0.009).
The OPUS-TIMI 16 trial showed the predictive relation between sCD40 ligands to CRP and troponin I. Risk for death and MI is increased even in patients with a low troponin I and elevated sCD40 or low CRP and elevated sCD40.
Placental growth factor
|
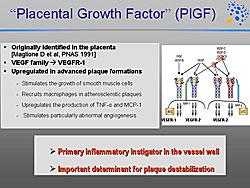
Placental growth factor belongs to the VEGF family, and is upregulated in advanced plaque formation, stimulates the growth of smooth muscle cells, recruits macrophages in atherosclerotic plaques, upregulates the production of TNF-alpha and MCP-1, and stimulates in particular abnormal angiogenesis (Figure 5). PIGF is thought to be the primary inflammatory instigator in the vessel wall, and therefore it is probably an important determinant for plaque de-stabilization.
In the CAPTURE population, they found that patients with elevated PIGF had the highest level of complications, compared to patients with low levels of PIGF. Interestingly, there was marked increases in the number of events as the level of PIGF increased. The diagnostic sensitivity and specificity for PIGF is clearly superior to that for CRP in the CAPTURE study. Combining markers again increased the predictive value. A low TnT and high PIGF level was associated with a 10.3% event rate for death and acute MI, and a high TnT and high PIGF was associated with a 31.4% event rate.
Multivariate analysis shows that the clinical markers of gender, age > 65 years, diabetes, creatine clearance, and ST segment depression lose their statistical significance. However, the biochemical markers remain significant, except for CRP, because the other markers are superior. TnT, sCD40, and PIGF are predictive for death and MI at 30 days.
Interleukin-10
This marker has a protective effect, and thus, the inflammatory balance between high interleukin-10 (IL-10) being protective and low CRP has been a topic of discussion.
The CAPTURE study showed that low IL-10 levels are associated with high event rates, while the higher protective levels of IL-10 are associated with lower event rates (about 8% vs 3%, respectively; adjusted hazard ratio 0.38; p=0.005).
A high CRP and high IL-10 levels are associated with a low event rate (about 6.8%), but a high CRP and a low IL-10 levels are associated with a high event rate (about 22%). A similar pattern is seen with TnT. A high TnT and a low IL-10 is associated with a 22% event rate, and a low TnT and a high IL-10 with a 4.6% event rate.
Summary
|
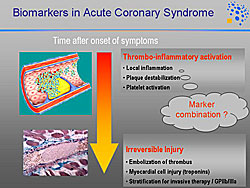
The ideal marker would precede irreversible cell injury, such as the embolization of thrombus that leads to irreversible cell injury marked by the release of troponin (Figure 6). Thus, markers of local inflammation, plaque destabilization, and platelet activation are needed. A combination of markers will most likely best stratify risk in patients with ACS.
Use of Biochemical Markers for Risk Stratification and Choice of Therapy in Acute Coronary Syndromes: Lessons from the FRISC II & GUSTO IV (+FRISC I & FAST) TrialsBertil LindahlUniversity of Uppsala
|
|
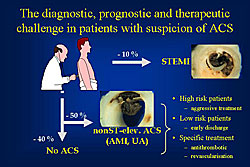
Patients admitted with suspicion of an acute coronary syndrome (ACS) constitute a diagnostic, prognostic and therapeutic challenge for the treating physician (Figure 1). Only about 10% of the patients admitted to the coronary care unit have an ST-segment elevation myocardial infarction (MI), which can be diagnosed solely on ECG, and biochemical markers are the basis for the diagnosis in the other 90%. About 20% will eventually be diagnosed as non-ST-segment elevation MI, 30% as unstable angina (UA), and in about 40% no ACS can be verified.
Results from FRISC II and GUSTO-IV
|
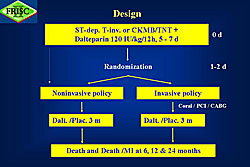
The factorial design of the FRISC II trial evaluated an early invasive versus a noninvasive approach, and evaluated long-term treatment with dalteparin versus placebo, over a 24-month follow-up (Figure 2). Patient inclusion was criteria were subjective symptoms and objective signs of ischemia (ST-T changes, CK-MB or troponin elevation). Patients were randomized as soon as possible after starting open-label dalteparin, and at least within 72 hours. The median time from onset of symptoms to randomization was 39 hours.
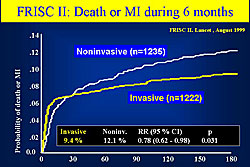
In FRISC II, there was a 22% relative reduction and a 2.7% absolute reduction in the composite endpoint of total death and MI (including those based on only elevation of biochemical markers). The early hazard of an invasive procedure was offset by the later gain based on the very low event rate after the procedures. The hazard curves crossed one another after around 30 days (Figure 3).
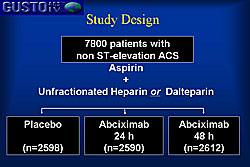
The GUSTO-IV trial, a large international multicenter trial in non-ST-elevation ACS, showed no benefit over placebo of an infusion of the GPIIb/IIIa inhibitor abciximab for 24 hours or 48 hours (Figure 4). Therefore the entire cohort of 7800 patients could be used for evaluation of different prognostic markers.
|
|
Prognostic value of troponins
Troponin T or troponin I are the preferred marker of myocardial damage, of the suggested markers and clinical variables for the early risk stratification of patients admitted with suspicion of ACS. Troponin elevation has consistently been shown by numerous studies to be associated with an increase in short-term and long-term risk of death and MI, with a linear increase in death as troponin increases.
A survival analysis from FRISC I showed troponin T levels were predictive of probable cardiac death. Troponin T level below 0.06 μg/L (no evidence of myocardial damage) was associated with a low probability of cardiac death, a troponin T between 0.06-0.6 had a significantly higher probability, and those with troponin T greater than 0.6 had the highest probability of cardiac death. The survival curves continued to separate during the whole follow-up period
However, the FRISC II and GUSTO-IV trials showed that for MI, a threshold effect seems to exist for the risk of a new MI—as soon as myocardial damage is present the risk of a new MI increases. Notably, the risk is largest in persons with minor damage and less in patients with major damage.
Much of the prognostic value of troponins in unstable coronary artery disease (CAD) can be attributed to the presence of underlying severe coronary stenosis. In patients without troponin elevation, no significant stenosis is common, but it is uncommon in patients without troponin elevation. Also common in patients with troponin elevation is 3-vessel disease, thrombosis of a culprit lesion that may cause downstream embolization or microinfarction, and, in some patients, total coronary occlusion and a large MI.
Predictive value of NT-proBNP
The standard 12-lead ECG remains the preferred ischemia marker, because it provides immediate information and is universally available. Plus, the degree of ST-segment depression gives additional information. The 1-year rate of death and MI is doubled in patients with ST-segment depression in 8 or more leads compared to patients with ST-depression in 4 or less leads.
Left ventricular (LV) function is probably the single most important predictor of mortality. The natriuretic peptides, BNP and NT-proBNP, have emerged as an easy and feasible way to assess cardiac performance by measuring a biochemical marker.
In the GUSTO-4 trial, there was a linear increase in mortality with an increase in NT-proBNP levels: an extremely low 1-year mortality of 0.4% in the lowest decile (NT-proBNP levels <98 ng/L) and an 27% mortality in the highest decile (NT-proBNP levels >4634 ng/L). Even within the normal range of NT-proBNP (<290), there seemed to be a gradual increase in mortality risk.
In GUSTO-IV, multivariable logistic regression analysis, adjusting for a large number of predictors for mortality, increasing quartiles of NT-proBNP independently contributed to the prediction of 1-year mortality. The odds ratio was greater than 3 for patients in the fourth quartile compared to the lowest quartile. The risk of a new, non-fatal MI was not associated with NT-proBNP levels, but was associated with troponin T levels, ST-segment depression, previous MI, and creatinine clearance.
Prognostic value of CRP
Of the increasing number of inflammatory markers shown to predict future cardiac events in ACS, the prognostic value of C-reactive protein (CRP) is best documented.
In FRISC, a survival analysis showed that patients in the highest tertile of CRP (>10 mg/L) had a higher probability of cardiac death compared to patients in the two lower tertiles, for which the survival curves are nearly super imposable. The survival curve for the highest tertile continues to separate from those for the two lower tertiles over the entire follow-up.
An independent association between CRP and ACS and short-term and long-term mortality has been shown in many trials. GUSTO-IV showed increasing short-term mortality with increasing quartiles of CRP—however, no association between CRP and the risk of a new MI.
Renal function
The importance of renal function has been emphasized in recent years. However, there are weaknesses related to measuring only creatinine, and calculating creatinine clearance is associated with several weaknesses and seldom done in clinical practice. Thus, cystatin C has emerged as an interesting marker of renal function.
Recently published results by Lindahl and colleagues from the FAST study confirmed the strong prognostic value of renal function and that cystatin-C levels, compared to creatinine clearance, better identify patients with low and high long-term mortality. Notably, even differences within the “normal” range of renal function were important prognostically.
Improving risk assessment
NT-proBNP, CRP, troponin T and creatinine clearance are independent predictors of mortality, and thus can be combined to further improve risk assessment.
In GUSTO-IV, the 1-year mortality was only 0.3% in the some 600 patients with an NT-proBNP level < 237 ng/L and a creatinine clearance > 84 ml/min. In contrast, the 1-year mortality was 25% in the some 400 patients with an NT-proBNP >1869 ng/L and a creatinine clearance < 51 ml/min.
Elevated troponin T levels, a marker of myocardial damage, also signals the need for intense anti-thrombotic treatment. This was first described by Lindahl and colleagues in the FRISC I study, where treatment with the low molecular weight heparin dalteparin was not beneficial in patients without elevated troponin T, but in contrast, in patients with elevated troponin T dalteparin prevented death or new MI. Now the same has been shown for other low molecular weight heparins and GPIIb/IIIa inhibitors.
In FRISC II, the beneficial effect of the invasive treatment, compared to a primarily noninvasive strategy, was confined to those patients with both troponin T elevation and ST-segment depression. In contrast, no beneficial effect was seen in patients with only troponin T elevation or only ST-segment depression. Similar results were demonstrated in the TACTICS-TIMI 18 trial.
There are few data on the use of BNP or NT-proBNP to determine treatment for ACS. However, results from FRISC II suggest that NT-proBNP may be useful for selecting treatment; the reduction in cardiac events with the invasive strategy was seen primarily in the patients in the upper tertile of NT-proBNP, although the interaction between NT-proBNP and effect of treatment did not reach statistical significance.
The FRISC risk score for death and MI comprises 4 clinical variables (age > 65 years, male gender, diabetes, prior MI), ECG, elevated troponin, and elevated IL-6 or CRP. In FRISC II, the invasive treatment was beneficial only in the patients with 3 or more of the factors in the risk score.
Summary
For early risk stratification, patient history, ECG, and levels of troponin T or I have been shown to be reliable, and in combination are useful to determine appropriate treatment. The level of BNP/NT-proBNP seems to add clinically relevant prognostic information.
Renal function should be incorporated in risk stratification strategies. A number of new inflammatory markers are promising, but their incremental prognostic value and clinical applicability remains uncertain.
Measurements of Cardiac Troponin T in Patients with Heart FailureYukihito SatoHyogo Prefectural Amagasaki Hospital
|
Symptoms of heart failure are subjective and interpretation of conventional tests in heart failure also may be subjective at times and sometimes complicated. Therefore, objective evaluation of patients with heart failure has been difficult to obtain. Biochemical markers are low cost and easy to measured, can be measured repeatedly, and are not susceptible to inter-observer variability. Thus, biochemical markers are ideal for the objective measurement of the heart failure syndrome.
The plasma measurement of brain natriuretic peptide (BNP) has been used increasingly for the diagnosis, prognosis, and monitoring of patients with congestive heart failure. However, is a single biochemical marker sufficient to evaluate heart failure, which is a complex syndrome.
Cardiac troponin T
Cardiac troponin T (cTnT) is a marker of myocyte injury in patients with heart failure.
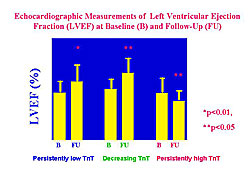
In 60 patients with dilated cardiomyopathy (DCM), with a mean follow-up of 16 months, 3 distinct patterns of serial measurement were identified: persistently high cTnT (≥0.02 ng/ml; n=17), initially high cTnT then decreased cTnT (decreasing cTnT; n=10), and persistently low cTnT (n=33).
Echocardiographic measurement of left ventricular (LV) ejection fraction (EF) at baseline and at follow-up in these patients showed that LVEF significantly increased in patients with persistently low cTnT and decreasing cTnT (Figure 1). However, LVEF significantly decreased in patients with persistently high cTnT.
In these patients, the adverse cardiac event-free (cardiac death, hospitalization for worsening heart failure) rate was significantly lower in the patients with persistently high cTnT than in the other two patterns (Figure 2).
|
|
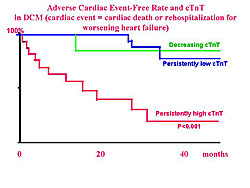
In patients with DCM, a subgroup of patients had persistently elevated cTnT concentrations, despite optimal therapy for heart failure, suggesting ongoing subclinical myocyte injury. The prognosis in these patients was poor.
Combined measurement of biochemical markers
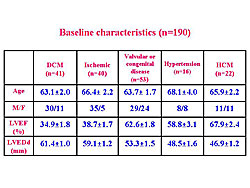
Sato and colleagues hypothesize that cTnT is a marker of myocyte injury and BNP is a marker of myocardial load. The baseline characteristics of 190 patients with heart failure in whom cTnT and BNP were measured simultaneously by Sato and colleagues is shown in Figure 3. The patients were similar except for a lower LVEF in patients with DCM and ischemic heart disease.
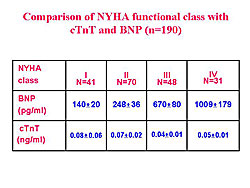
A comparison of these patients based on New York Heart Association (NYHA) functional class showed a step-wise increase in both NYHA class and BNP, however, cTnT levels were identical in each NYHA class (Figure 4).
|
|
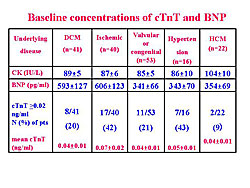
They also showed that for each underlying disease, CK levels were the same for the baseline levels of cTnT and BNP (Figure 5). BNP was significantly elevated in patients with DCM and ischemic heart disease. Elevated cTnT levels were found in 10-40% of patients in the various disease categories.
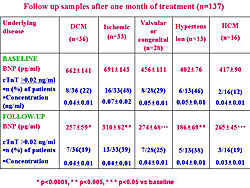
In 137 of the patients who were evaluated at 1 month after treatment for heart failure, the BNP concentrations decreased significantly in all the disease categories (Figure 6). However, most of the patients who had elevated cTnT levels at baseline had persistently increased cTnT levels at the 1 month follow-up. Also, cTnT levels were identical in each disease category.
|
|
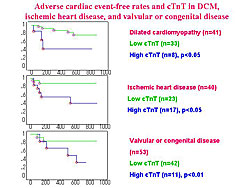
The adverse cardiac event-free rate in the 190 patients was significantly lower in patients with a high cTnT than in patients with a low cTnT (Figure 7). This was observed in each disease category.
In patients with a high cTnT and a low BNP, no myocardial overload was observed. However, subclinical myocyte injury is ongoing. In patients with a low cTnT and a high BNP, heart failure is present in the absence of ongoing myocyte injury. Patients with a high cTnT and high BNP had the worst prognosis (Figure 8).
|
|
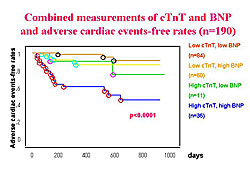
In summary, elevated cTnT concentrations were found in 10-40% of patients with a variety of heart failure diseases. cTnT did not correlate with NYHA functional class. After 1 month of treatment, BNP decreased significantly. However, most patients with elevated cTnT at baseline, had persistently elevated concentrations of cTnT. Patients with elevated cTnT had a worse prognosis than patients with a low cTnT. Patients with elevated concentrations of both cTnT and BNP had the poorest prognosis.
Relation between cTnT and other biomarkers
Based on their preliminary data, Sato and colleagues hypothesize that hemodynamic stress, cytokines, metabolic stress, and extracellular matrix changes may affect myocyte injury. BNP, renin, epinephrine, norepinephrine, CRP, among others, were elevated in patients with high levels of cTnT compared to low levels of cTnT. On multivariate analysis, cTnT, BNP, norepinephrine, CRP, and type 1 collagen were independent prognostic factors of cardiac events in patients with heart failure.
Conclusions
In the future, the identification of myocyte injury at early stage of disease, characterized by the presence of risk factors, such as hypertension, diabetes, hyperlipidemia, etc. is needed. Therapeutic monitoring with bedside rapid assays in the setting of acute cardiac decompensation is needed. Thus, this group anticipates that both cTnT and BNP will become standard tests in the management of heart failure.
|
|
| Copyright © 2005 Japanese Circulation Society All Rights Reserved. webmaster@j-circ.or.jp |